Anterior Open Bite and Aligners: Protocol, Intrusion and Relapse Risk

Complete clinical guide to managing anterior open bite with clear aligners: differential diagnosis, intrusion biomechanics, vertical attachments and retention strategies.
Anterior open bite is one of the most complex malocclusions to manage in orthodontics. It is also among the most relapse-prone, regardless of the treatment modality used. Long considered a relative contraindication to clear aligners, it is now successfully managed by practitioners who have mastered the specific biomechanics of posterior intrusion and anterior extrusion. This clinical guide details the protocol, indications, limitations and retention strategies.
1. Differential Diagnosis — Identifying Aetiology Before Planning
Not all anterior open bites are equal and the treatment protocol depends directly on their aetiological mechanism. Three main origins are distinguished: skeletal open bite (posterior vertical excess, hyperdivergence, open mandibular angle), dental open bite (molar suprusion, incisor infraclusion without major skeletal component) and habit-related open bite (atypical swallowing, thumb-sucking, tongue interposition). The distinction is critical: a pronounced skeletal open bite (SN-GoGn > 38°, gonial angle > 135°) exceeds the scope of aligners alone and requires a surgical discussion. Before any planning, a complete cephalometric analysis is mandatory.
- Lateral cephalogram + Björk-Jarabak analysis (mandibular rotation)
- Mandibular plane angle (FMA): > 30° = significant skeletal component
- Lower facial height (ANS-Me / N-Me): ratio > 57% = high risk
- Tongue interposition assessment: clinical swallowing test
- Intraoral photographs + digital models with segmental overbite measurement
2. Indications and Contraindications for Aligners
Clear aligners are a valid therapeutic option for anterior open bites of predominantly dental origin with moderate skeletal component. Ideal cases are open bites under 4 mm, mandibular angle within high norms (FMA 28–34°), isolated habitual or dental aetiology, and adult patients with completed growth. Conversely, relative contraindications include: open bite greater than 5–6 mm, pronounced hyperdivergence with elevated lower facial ratio, active growth (adolescent patient) and above all an uncorrected oral habit — treatment will inevitably relapse if the habitual aetiology is not simultaneously addressed.
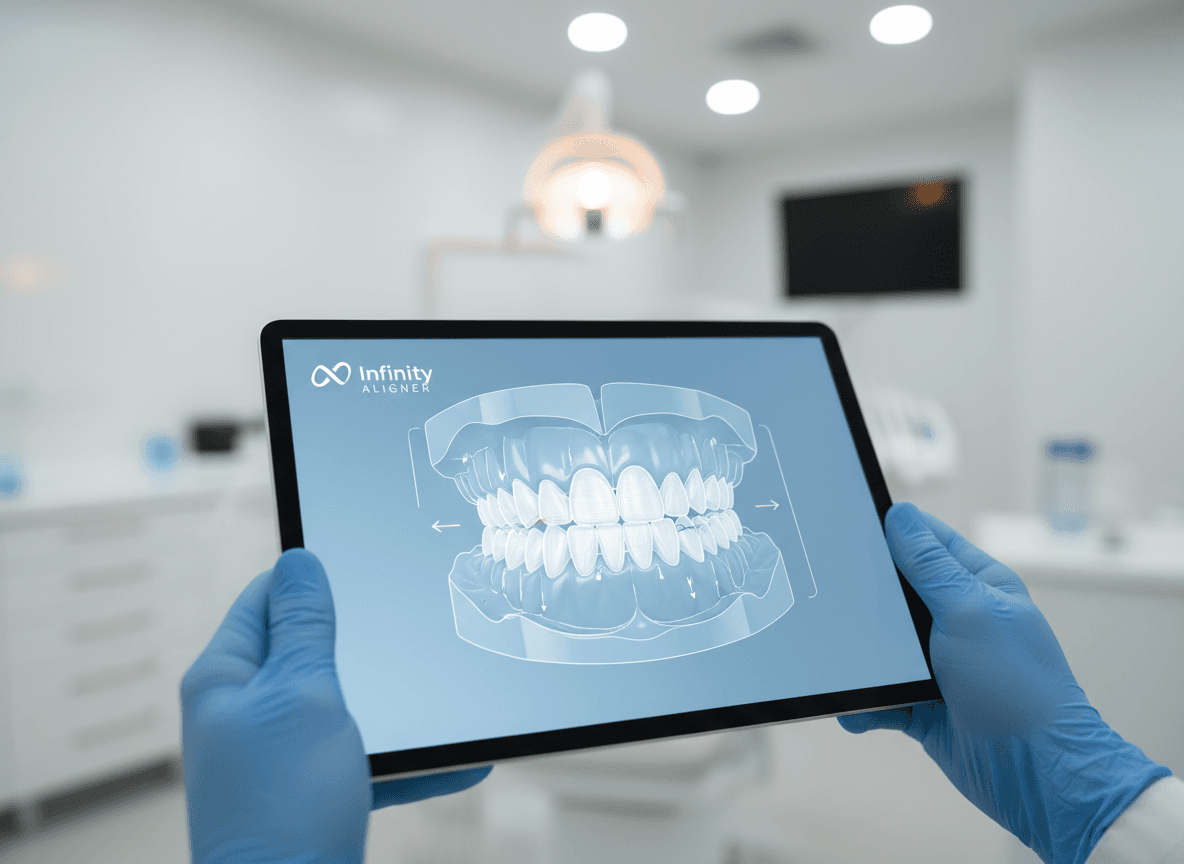
3. Correction Biomechanics — Two Complementary Mechanisms
Closure of an anterior open bite with aligners relies on two distinct biomechanical vectors, generally used in combination: posterior intrusion and anterior extrusion. Intrusion of posterior segments — particularly premolars and molars — produces an anticlockwise mandibular rotation (angle closure) that mechanically reduces anterior open bite. This is the most powerful and stable mechanism over time. Extrusion of anterior incisors and canines completes closure by bringing incisal edges downward to establish contact. This second mechanism, while more direct, is biomechanically less stable and more exposed to relapse, particularly in cases of residual tongue interposition.
3.1 Posterior Intrusion — Activation Protocol
Posterior segment intrusion with aligners is facilitated by their full occlusal surface envelopment geometry. Unlike brackets, the aligner exerts an intrusion force distributed across the entire coronal surface, reducing the risk of uncontrolled torque. To maximise efficiency: prescribe intrusion movements of 0.1–0.15 mm per stage (no more), place vertical attachments on upper first molars to improve intrusion axis control, and avoid simultaneous expansion sequences that risk counteracting intrusion with a parasitic extrusion component. The number of stages required to obtain 1 mm of real molar intrusion averages 8–12 stages, due to the underexpression of intrusion movements inherent to aligners.
3.2 Anterior Extrusion — Limitations and Precautions
Extrusion of anterior teeth is one of the movements least well expressed by aligners — with a real expression rate estimated at 30–40% of theoretical prescription according to the literature. To improve this expression, extrusion attachments (rectangular, horizontal, on the buccal surface) are essential from the first stages. Prescription must be overcompensated: if you want 2 mm of real extrusion, plan 4–5 mm in the simulation. Additionally, monitor root torque control during extrusion: uncontrolled upper incisor extrusion can lead to progressive labial tipping that worsens anterior protrusion and compromises the aesthetic result.
4. Attachment Plan and Auxiliaries — Recommended Clinical Configuration
The attachment plan is critical in open bite management. Generic prescription is insufficient — each case requires individualised consideration of type, size and position of attachments.
| Zone | Recommended Attachment | Biomechanical Objective | Precaution |
|---|---|---|---|
| Upper incisors | Horizontal rectangular, buccal surface, cervical third | Extrusion + torque control | Avoid incisal third — early debonding risk |
| Upper canines | Vertical rectangular or rotation-optimised | Anchorage + extrusion axis control | Verify available crown height |
| Upper premolars | Vertical rectangular, mesial surface | Anchorage for posterior intrusion | Essential — without it, intrusion is poorly controlled |
| Upper first molars | Vertical rectangular, mesio-buccal surface | Intrusion control + tip resistance | Watch gingival height — avoid furcation zone |
| Lower incisor segment | Horizontal rectangular if extrusion prescribed | Lower step closure | Optional depending on open bite severity |
5. Vertical Elastics — Integration into the Aligner Protocol
For open bites greater than 3 mm or in cases of insufficient extrusion movement expression, vertical intermaxillary elastics are an indispensable auxiliary. They are worn through precision cutouts made in the aligners, positioned at canine-to-canine or premolar-to-premolar hooks depending on the open bite geography. Recommended force is 60–100 g per side (3/16 inch elastics, light to medium force). Wear must be prescribed full-time (22h/24) during the active closure phase. Non-compliance with elastics is the primary cause of underresult in this case type — discuss this explicitly with the patient before treatment begins.
6. Relapse Risk — Understanding the Mechanisms to Prevent Them
Anterior open bite has the highest relapse rate of all orthodontic malocclusions, across all treatment systems. Long-term studies (follow-up > 5 years) report partial or total relapse rates ranging from 25 to 45% depending on the cohort. The mechanisms involved are multiple and often interrelated.
- Persistent tongue interposition (primary cause — relapse inevitable if not corrected)
- Residual growth in a hyperdivergent direction in adolescents
- Alveolar crest resorption after excessive molar intrusion
- Rebound of extruded teeth in the absence of appropriate retention
- Resumption of oral habits (atypical swallowing, untreated mouth breathing)
- Failure to wear removable nocturnal retention beyond 12 months
7. Retention Strategies — Open Bite-Specific Post-Treatment Protocol
Post-treatment retention for open bite requires a more rigorous protocol than for conventional malocclusions. Standard retention (removable nocturnal retainer alone) is insufficient in the majority of cases. The recommended protocol systematically combines bonded anterior retention (braided wire 3–3 on both arches) with a thermoformed night retainer worn for life. The night retainer must cover the posterior segment to maintain the molar intrusion level achieved — a retainer covering only the anterior teeth is counterproductive in this context. Clinical and photographic follow-up at 6, 12 and 24 months post-treatment is mandatory to detect early emerging relapse before it becomes clinically significant.
8. Multidisciplinary Coordination — Speech Therapy and Myofunctional Treatment
For open bites of habitual or myofunctional origin, speech therapy and myofunctional rehabilitation is a sine qua non condition for long-term stability. It should ideally be initiated before or at the start of orthodontic treatment — never after the retention phase. The objective is normalisation of the swallowing pattern (somatic swallowing, lip-to-lip contact), lingual posture at rest (tongue tip on the palatal papilla, not the incisors) and nasal breathing. Without this rehabilitation, the most technically accomplished orthodontic treatment will result in relapse within 18–36 months post-retention.
Key Takeaways
- Aetiological diagnosis (skeletal vs dental vs habitual) entirely conditions the indication for aligners.
- Posterior intrusion is the most stable mechanism — anterior extrusion must be overcompensated (×2 to ×2.5).
- Attachments on premolars and molars are non-negotiable for controlling intrusion.
- Vertical elastics are essential for any open bite > 3 mm.
- Relapse rate is 25–45% at 5 years — retention must be double (bonded + removable) and maintained for life.
- Without myofunctional rehabilitation in habitual aetiology cases, relapse is near-certain.
- Photographic follow-up at 6, 12 and 24 months post-treatment is mandatory.
Infinity Aligner
Clinical & editorial team
More articles

How to Choose Clear Aligners in Tunisia

Clear Aligners vs Braces: Complete Comparison

How Much Do Clear Aligners Cost in Tunisia?
How Long Does Clear Aligner Treatment Take?

How to Clean and Care for Your Clear Aligners Daily

Clear Aligners for Teenagers: What Parents Need to Know
Gap Teeth & Diastema: Can Clear Aligners Fix Them?
Can You Play Sports with Clear Aligners?

3D Smile Simulation: How It Works and What to Expect

Orthodontic Relapse: Why Teeth Move After Treatment
Intraoral Scanner vs Traditional Impressions: What's the Difference?

Clear Aligners for Adults: Is It Ever Too Late?

Wisdom Teeth and Clear Aligners: Are They Compatible?

Clear Aligners: A Versatile Therapeutic Approach in Orthodontics

Orthodontics and Periodontal Health: What Every Patient Needs to Know

The Technology Behind Clear Aligners: From Design to Tray

How to Prepare for Your Orthodontic Consultation: 10 Questions to Ask

Bruxism and Clear Aligners: Can You Correct and Protect at the Same Time?

Class II Malocclusion and Clear Aligners: What Treatment Options Exist?

Clear Aligners and Dental Implants: Protocol, Timing and Clinical Cases

Digital Workflow and Aligner Biomechanics: The Advanced Practitioner Protocol

The Limits of Clear Aligners: Identifying Complex Cases Beyond Their Reach

Aligner Manufacturing: Thermoforming, 3D Printing and Polymer Science

Invisible Orthodontics in 2030: Predictive AI, Direct Printing and Active Materials

Smile Without Borders: The Price of Aligners Between Tunisia, Europe and Canada
Attachments in Invisible Orthodontics: The Silent Levers of Biomechanics

The Smile Beyond the Mirror: The Profound Impact of Dental Alignment on Psychological Well-being

Tunisia: The New Eldorado of Digital Dentistry and Medical Tourism
Post-Orthodontic Retention: The Forgotten Step That Decides Everything
What You Can (and Cannot) Eat With Clear Aligners

Teeth Whitening and Clear Aligners: Can You Treat and Whiten at the Same Time?
TMJ and Clear Aligners: How Invisible Orthodontics Acts on Jaw Pain
The Different Types of Dental Retainer: A Complete Guide After Orthodontic Treatment

The hidden dangers of metal braces: what patients need to know

Root resorption: the silent risk of poorly managed orthodontic treatments

Orthodontics and cavities: how metal braces compromise dental hygiene

Orthodontic relapse: why teeth return to their original position

Braces and chronic pain: the underestimated impact on daily quality of life
Intraoral scanner vs conventional impressions: dimensional analysis and clinical implications

CAD/CAM digital workflow in orthodontics: from intraoral scanning to aligner fabrication
Deformation, shrinkage and cumulative errors: why the conventional impression chain compromises aligner precision
Intraoral Scanners 2025: Complete Technical and Metrological Comparison
Why Choose Infinity Aligner? The Complete Guide for Dental Practitioners

Composite Selection for Aligner Attachments: Mechanical Analysis and Clinical Protocol

TMJ and Malocclusion: Differential Diagnosis and Clinical Approach for the Practitioner

Travelling with Clear Aligners: The Complete Guide for Stress-Free Trips
The First Month with Aligners: What to Expect Week by Week

Pre-Prosthetic Orthodontics: Preparing the Site Before Implants or Veneers

How to Present Aligners to a Hesitant Patient — A Consultation Script
Posterior & Anterior Crossbite: Diagnosis and Correction with Clear Aligners
Consult a certified dentist
Our 200+ certified partners in Tunis, Sfax, Sousse and the francophone zone welcome you.
Book a consultation